Medication is one of the core treatments for ADD/ADHD and has a history in child psychiatry going back over fifty years. Although stimulant medications (called stimulants because they cause stimulation in non-ADD/ADHD persons and, paradoxically, the opposite in those with the disorder(s)), are by far the most effective and widely used drugs, currently the treatment of ADD/ADHD also includes other classes of psychotropic medications. These are far less effective but might be necessary when stimulants alone don’t work or cannot be tolerated. These include some antidepressants and blood pressure medications.
ADD/ADHD medications have received a lot of publicity over the years, mostly because of the millions of children who have received them. Reports have ranged from raves about their effectiveness to diatribes against their safety that instill the fear of death in parents. In fact, these medications are the most widely used in child psychiatry and have been the most studied, so they are some of the safest medications out there, although there are some side effects which are usually transient and mild. The stimulants are not only effective agents to treat ADD/ADHD, but also work quickly.
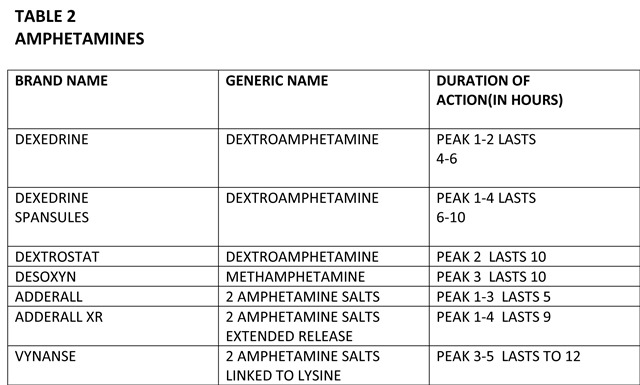
There are two major classes of stimulant medications; methylphenidate (i.e. Ritalin) and its derivatives, and amphetamine (i.e. Adderall) and its derivatives. (See lists below).
All the stimulants are approved for children six years old and over. Adderall, Dexedrine, and Dextrostat are also approved for children as young as three years old. Having said that, each psychiatrist develops his own style for prescribing within the overall safe parameters of the profession, and personally, I try to be as flexible as possible and make sure that the parents and the children that I work with understand why I am prescribing the medication and all the possible complications involved with it. My goal is to decrease the resistance or fear. The important thing is for parents to do their homework and to understand actually what these drugs can and cannot do.

DISCLAIMER
Information contained in this blog is intended for educational purposes only. It is not intended as medical or psychiatric advice for individual conditions or treatment and does not substitute for a medical or psychiatric examination. A psychiatrist must make a determination about any treatment or prescription. Dr. Paul does not assume any responsibility or risk for the use of any information contained within this blog.
